We all remember blood flow through the heart being pounded into our heads in school. Knowing the blood flow through the brain is every bit as important and proficiency in the basics of cerebral vasculature can quickly improve your assessment of stroke patients. There is a concept in stroke diagnosis known as localization. This refers to connecting the pattern of a patient’s symptoms back to the location where the clot might be lodged. An experienced physician can often determine the area of the brain involved in the stroke and the vessel which is occluded based off of a physical assessment.
For EMS, knowing the anatomy & common presentation patterns (or syndromes) can help a medic further his/her understanding of stroke pathophysiology & severity.
Let’s look at a couple of pictures to help visualize the anatomy. Don’t get too caught up in all the vessels…there are only a couple we will be discussing for now: the Carotid Arteries, the Basilar Artery, the Vertebral Arteries, the Circle of Willis, and the Right & Left Middle Cerebral Arteries.
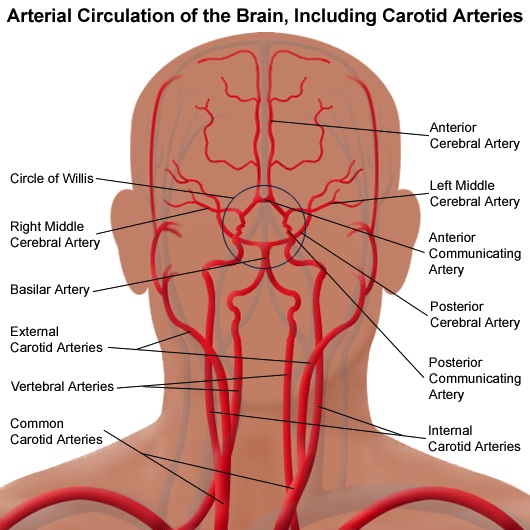
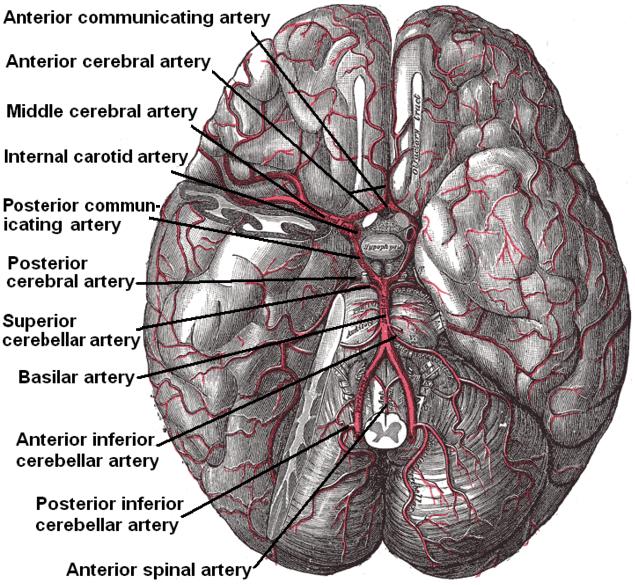
Take a moment and make sure you can identify exactly where the above-mentioned vasculature is located. Don’t worry about any of the others yet.
The picture on the top is a view as if you were standing face to face with someone while the view on the bottom is what you would see if you were standing directly on top of the heart tilting your head back and looking up towards the brain.
Let’s take a closer look at the mentioned structures starting with the carotids. Somewhere about the level of the thyroid cartilage the carotid arteries bifurcate into the interior and exterior carotids. The exterior go on to provide circulation to the face while the interior continue upwards to the brain. The internal carotids form the anterior circulation of the brain. The vast majority of strokes occur in the anterior vasculature.
The vertebral arteries arise from the subclavian arteries (underneath the clavicles) and continue up along the spinal cord merging together to become the basilar artery. These vessels account for theposterior circulation of the brain.
The carotids and the vertebrobasilar connect together and form an amazing structure called the Circle of Willis. This is a large circular structure sitting beneath the brain which creates the blood supply of the brain and feeds arteries which branch out from it. One of the unique facets of the Circle of Willis’ design is that if the vertebrobasilar arteries cease functioning there is still some supply of blood being circulated around from the carotids (and vice versa). This helps to ensure continued blood flow.
There are two main vessels which arise from the Circle of Willis: the right & left Middle Cerebral Arteries. The MCA supplies the vast majority of the brain’s blood supply and by virtue accounts for a significant number of strokes. The Right MCA branches off and feeds the right side of the brain whereas the Left MCA branches off and feeds the left side.
To circle back around to the concept of localization let’s consider the case of a 90 year old female presenting with complete left-side hemiparesis, left-side facial paralysis, left-side vision loss, left-side neglect, and significant dysarthria. Where is the stroke likely to be occurring?
Remember that motor function is controlled by the opposite side of the brain. If our patient presents with left-sided deficit then we can start looking to the right side of the brain. Now let’s use what we just learned about vasculature to narrow down the likely location.
We have the complete loss of function to the left side which indicates that this is a severe stroke and indicative of a complete loss of the blood supply since absolutely nothing is presently working. [Consider as the blood supply begins to slow, full function turns to numbness, which turns to weakness, which worsens until full paralysis is achieved when blood flow ceases. The symptoms on numbness, weakness, and paralysis can help us understand the severity of the stroke and the amount of the vessel which has become blocked.]
Since we know the Circle of Willis helps to provide some continued blood flow, it is unlikely that the occlusion is occurring at this level or lower. We can think about ruling out the Circle of Willis, the vertebrobasilar arteries, and the carotids. This leaves us with the Middle Cerebral Arteries. Since our patient is symptomatic on the left side, and motor control is opposite, we are looking at the Right MCA as the culprit. In fact, this patient’s presentation is classic Right MCA Syndrome. Flip the symptoms to the other side and we would be thinking about Left MCA Syndrome.
Of course, stroke pathophysiology and localization is complex and requires years of dedicated training to master but hopefully this gives you a greater understanding of the cerebral vasculature and how strokes present. There are a multitude of syndromes and varying degrees of severity but the Right & Left MCA syndromes are the classic patterns which we teach EMS providers to look for. Remember that complete acute loss of function compared to the varying degrees of acute weakness can reveal how much of the blood supply has been cut off.
Look for more in this series as we dive further in depth with the cerebral vasculature!
![]()








4 Trackbacks